
Overview
Testicular torsion is a relatively uncommon presentation within regular general practice but has a suggested prevalence of 1 in 4,000 in males under the age of 25. It appears with greater frequency within providers of unscheduled care because of its relatively sudden and severity of presentation. It can be difficult to recognise clinically and can be intermittent in its presentation as the testes twist and spontaneously untwist. Once recognised it is a surgical emergency with a 6 hour window for testes preserving surgery.
Signs and Symptoms
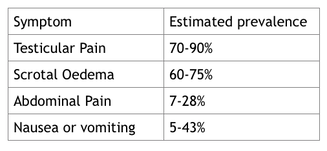
These are variable testicular pain is not a universal finding and can be absent or intermittent. Swelling of the scrotum or testes, oedema and redness of scrotal skin or abdominal pain may all be features. It is important that the scrotum is carefully examined in the distressed male infant where no other cause is identified.
Typically the pain should be severe and sudden onset, possibly radiating to the groin or lower abdomen, it can be accompanied by vomiting nausea and dysuria. It may be proceeded by low grade trauma to the testes and should be considered where there is no history of urinary tract or Genito urinary infection
Testicular torsion is a relatively uncommon presentation within regular general practice but has a suggested prevalence of 1 in 4,000 in males under the age of 25. It appears with greater frequency within providers of unscheduled care because of its relatively sudden and severity of presentation. It can be difficult to recognise clinically and can be intermittent in its presentation as the testes twist and spontaneously untwist. Once recognised it is a surgical emergency with a 6 hour window for testes preserving surgery.
Signs and Symptoms
These are variable testicular pain is not a universal finding and can be absent or intermittent. Swelling of the scrotum or testes, oedema and redness of scrotal skin or abdominal pain may all be features. It is important that the scrotum is carefully examined in the distressed male infant where no other cause is identified.
Typically the pain should be severe and sudden onset, possibly radiating to the groin or lower abdomen, it can be accompanied by vomiting nausea and dysuria. It may be proceeded by low grade trauma to the testes and should be considered where there is no history of urinary tract or Genito urinary infection
Signs are of limited value in excluding the diagnosis, though the presence of a transverse high lying testes or abnormal position compared with the alternate side may support clinical suspicion.
Actions
Testicular torsion is a surgical emergency with testicular salvage possible in 90-100% of cases operated on within 6 hours of onset of symptoms, this drops to 20-50% at 12 hours after onset. Orchidectomy or subsequent testicular atrophy results in 5-50%
Patients should be referred for urgent assessment and kept nil by mouth until a torsion has been excluded in hospital.
Summary
- Testicular torsion may be difficult to diagnose if symptoms are intermittent or atypical, but it must be considered in all cases of scrotal pain, with careful history and examination.
- Sudden, severe onset of testicular pain with tenderness should be considered as torsion and referred, unless other clinical features suggest an alternative diagnosis.
- Examine the testis for tenderness, size, shape, and position, and examine the remaining scrotal contents, comparing findings with the unaffected side.
Case Study
https://www.themdu.com/guidance-and-advice/case-studies/testicular-torsion
Learning resources.
https://bestpractice.bmj.com/topics/en-gb/506
https://learning.bmj.com/learning/module-intro/testicular-torsion.html?moduleId=10029430&searchTerm=“testicular torsion”&page=1&locale=en_GB
Further Reading
Testicular Torsion
1. Somani BK, Watson G, Townell N. Testicular torsion. BMJ (Clinical research ed) 2010; 341.
Download the PDF.
 RSS Feed
RSS Feed