
Overview
Sepsis is responsible for ~37,000 deaths a year in England, with 123,000 cases annually1. Sepsis can be difficult to spot and good GPs “Miss It”. Sepsis is defined as “life threatening organ dysfunction caused by a dysregulated host response to an infection2” and is a time critical medical emergency. The mortality of Septic Shock increases 8% with every hour that passes without initiation of iv antibiotics3. If recognised early it can be treated effectively with oxygen, fluids, and antibiotics4.
Signs and Symptoms
Infection is a common cause of ill health but there are few pathognomonic signs or symptoms specific to deteriorating infection or sepsis. NICE list symptoms that may alert to the possibility but over triage significantly in most locations.( Appendix A).
Assessing Adults
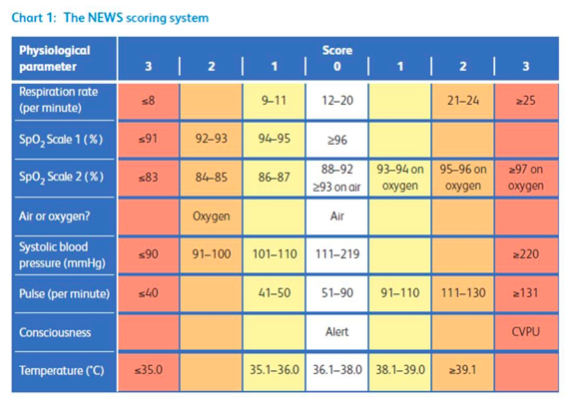
The presence of sepsis is most commonly indicated by a history of deterioration in the presence of possible infection, clinical judgement and abnormal physiology. The assessment of physiology should include respiratory rate, blood pressure/perfusion, oximetry, pulse and temperature, with a judgement made about cognition. We know that the presence of abnormal respiratory rate, reduced blood pressure and altered cognition are the best predictors of sepsis particularly in combination. In hospital abnormal values for these variables are assessed against a NEWS Score using the table below to calculate an aggregated score. The predictive value of NEWS in Primary care is yet to be determined, but we know that patients presenting in the ED with a NEWS score of 3 or less have a low chance of having sepsis, and that a score of 5 or above is strongly suggestive of sepsis in the presence of probable infection.
Sepsis is responsible for ~37,000 deaths a year in England, with 123,000 cases annually1. Sepsis can be difficult to spot and good GPs “Miss It”. Sepsis is defined as “life threatening organ dysfunction caused by a dysregulated host response to an infection2” and is a time critical medical emergency. The mortality of Septic Shock increases 8% with every hour that passes without initiation of iv antibiotics3. If recognised early it can be treated effectively with oxygen, fluids, and antibiotics4.
Signs and Symptoms
Infection is a common cause of ill health but there are few pathognomonic signs or symptoms specific to deteriorating infection or sepsis. NICE list symptoms that may alert to the possibility but over triage significantly in most locations.( Appendix A).
Assessing Adults
The presence of sepsis is most commonly indicated by a history of deterioration in the presence of possible infection, clinical judgement and abnormal physiology. The assessment of physiology should include respiratory rate, blood pressure/perfusion, oximetry, pulse and temperature, with a judgement made about cognition. We know that the presence of abnormal respiratory rate, reduced blood pressure and altered cognition are the best predictors of sepsis particularly in combination. In hospital abnormal values for these variables are assessed against a NEWS Score using the table below to calculate an aggregated score. The predictive value of NEWS in Primary care is yet to be determined, but we know that patients presenting in the ED with a NEWS score of 3 or less have a low chance of having sepsis, and that a score of 5 or above is strongly suggestive of sepsis in the presence of probable infection.
 | For GPs this amounts to identifying a deteriorating patient with possible/probable infection using clinical judgement and augmenting that decision making by assessing physiology. When a decision is made to admit this should be done by the clinician calling 999, stating that they “Suspect Sepsis” and being prepared to give the NEWS Score or the abnormal physiology of concern. |
In patients where sepsis is not suspected but infection is a possible or probable cause of being unwell they should have some recorded assessment of respiratory rate/effort, perfusion, and cognition. They or their carers should also receive specific safety netting as to the signs of sepsis, and ideally an age appropriate Sepsis leaflet.
Assessing Children
This can present a significant clinical challenge. Children’s physiology can vary wildly according to age and their response to infection. There is no standardisation of Paediatric Early Warning Scores as yet and the values they contain are validated against different cohorts of children to those seen in Primary care. There is also no standard paediatric definition of what determines the presence or absence of sepsis.
None of this helps the General Practice clinician. Clinical assessment should include judgement as to the history and unusual signs, including rashes abnormal alertness, clinician and parental concern. It should also contain a record of an assessment of physiology, particularly their respiratory rate/distress, perfusion (capillary refill, pulse rate) and level of cognition/social interaction. In many children this may be represented as negative findings, (no respiratory distress, pink and playing with toys, running around room or smiling appropriately). Temperature alone is a poor predictor of wellness. The more unwell the child the more formal the assessment may need to be, particularly where the judgement is to keep the child at home.
Safety netting for children needs to be better than “if they get worse come back” and should include some indication of what worse looks like. This should be supported by an age appropriate leaflet.
Verbal advice for Parents of Children with Infection
Your child has xxx infection and is likely to improve with/without treatment. Very occasionally they can get significantly worse, signs of getting worse can include:
If these occur then you should consider getting your child assessed as a matter of urgency.
Summary
Further Reading
E-Learning for Health Sepsis Modules
RCGP Sepsis: Guidance for GPs
References
1. Hospital Episode Statistics: Health and Social Care Information Centre. 2015. http://www.parliament.uk/business/publications/written-questions-answers-statements/written-question/Commons/2015-09-16/10526/.
2. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Jama 2016; 315(8): 801-10.
3. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Critical care medicine 2006; 34(6): 1589-96.
4. Daniels R. Surviving the first hours in sepsis: getting the basics right (an intensivist's perspective). The Journal of antimicrobial chemotherapy 2011; 66 Suppl 2: ii11-23.
Appendix A
NICE Guidance
Assessing Children
This can present a significant clinical challenge. Children’s physiology can vary wildly according to age and their response to infection. There is no standardisation of Paediatric Early Warning Scores as yet and the values they contain are validated against different cohorts of children to those seen in Primary care. There is also no standard paediatric definition of what determines the presence or absence of sepsis.
None of this helps the General Practice clinician. Clinical assessment should include judgement as to the history and unusual signs, including rashes abnormal alertness, clinician and parental concern. It should also contain a record of an assessment of physiology, particularly their respiratory rate/distress, perfusion (capillary refill, pulse rate) and level of cognition/social interaction. In many children this may be represented as negative findings, (no respiratory distress, pink and playing with toys, running around room or smiling appropriately). Temperature alone is a poor predictor of wellness. The more unwell the child the more formal the assessment may need to be, particularly where the judgement is to keep the child at home.
Safety netting for children needs to be better than “if they get worse come back” and should include some indication of what worse looks like. This should be supported by an age appropriate leaflet.
Verbal advice for Parents of Children with Infection
Your child has xxx infection and is likely to improve with/without treatment. Very occasionally they can get significantly worse, signs of getting worse can include:
- Becoming increasingly breathless
- Pale and clammy “the colour someone goes when they are about to be sick”
- Unnaturally drowsy or unresponsive
- Not passing urine in the previous 12 hours.
If these occur then you should consider getting your child assessed as a matter of urgency.
Summary
- When assessing any patient with infection consider if there are features that might suggest sepsis and document their presence or absence
- Assessment of Respiratory Rate, Blood Pressure/perfusion and cognition should all be assessed and recorded for all patients with infection
- National Early Warning Score (2017) should be considered to be the bench mark for abnormal values in adults.
- Paediatric Early Warning scores and NICE Guidance vary in their contents and values but all provide an indication of abnormal values. Clinical and parental judgement remains a strong predictors
- Oximetry should be recorded using age appropriate devices and probes
- Escalation to ambulance or other services should be done by the clinician and must include the phrase “Suspected Sepsis” and give a NEWS score in adults and abnormal physiological findings in children
- Safety Netting should be sepsis specific supported by age appropriate leaflets.
Further Reading
E-Learning for Health Sepsis Modules
RCGP Sepsis: Guidance for GPs
References
1. Hospital Episode Statistics: Health and Social Care Information Centre. 2015. http://www.parliament.uk/business/publications/written-questions-answers-statements/written-question/Commons/2015-09-16/10526/.
2. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Jama 2016; 315(8): 801-10.
3. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Critical care medicine 2006; 34(6): 1589-96.
4. Daniels R. Surviving the first hours in sepsis: getting the basics right (an intensivist's perspective). The Journal of antimicrobial chemotherapy 2011; 66 Suppl 2: ii11-23.
Appendix A
NICE Guidance
Table 1: Risk stratification tools for adults, children and young people aged 12 years and over with suspected sepsis
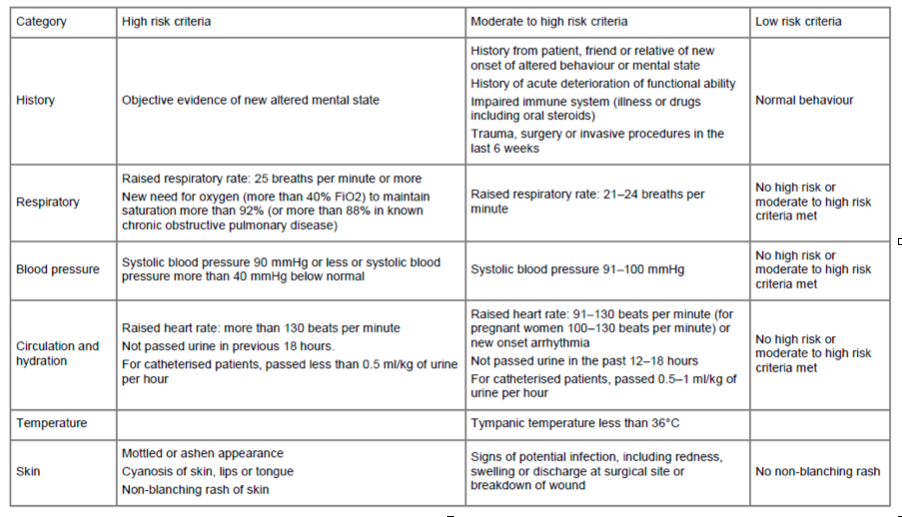
Table 2: Risk stratification tool for children aged 5-11 years with suspected sepsis
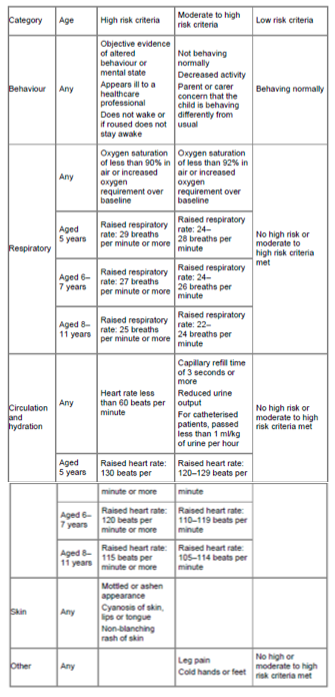
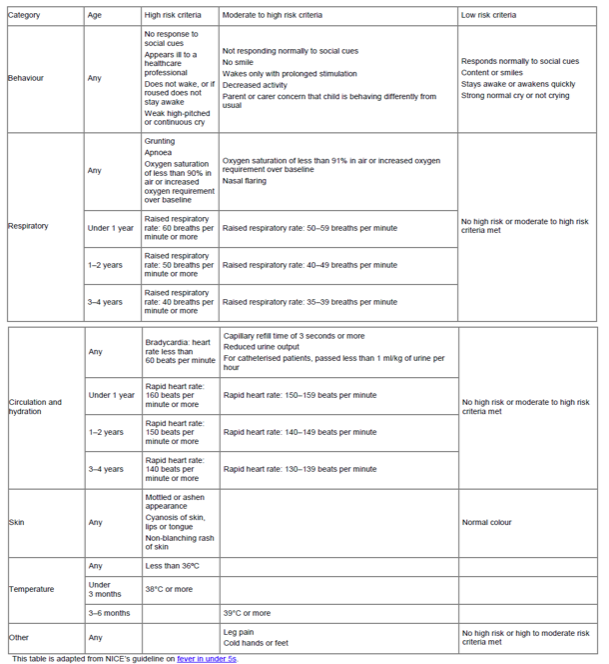
Table 3: Risk stratification tool for children aged under 5 years with suspected sepsis
 RSS Feed
RSS Feed